






 i
iIntroduction
Site neutral payment proposals may affect access differently across patient populations. In this +Insight, we focus on how site-of-service patterns for drug administration services, which both the Medicare Payment Advisory Commission (MedPAC) and Congress have singled out for potential site neutral payment reductions, differ for Medicare beneficiaries living in rural and urban areas and how it can affect access to care.
We have focused on site neutral payment proposals in previous +Insights, including our June 2023 +Insight on the services likely to be impacted if MedPAC’s recent site neutral payment proposal is enacted, and our February 2024 +Insight on how site-of-service patterns vary across individual procedure codes that map to the same ambulatory payment classification.
The outpatient prospective payment system includes four ambulatory payment classifications (APCs) for drug administration services.1 MedPAC has recommended that all four of these APCs be subject to site neutral payment reductions, and all four were targeted for site neutral payment reductions by Congress in the Lower Costs, More Transparency Act (H.R. 5378).2
To understand how site neutral payments for drug administration services could impact access to care for beneficiaries based on where they live, we analyzed Medicare fee-for-service (FFS) claims billed by hospital outpatient departments (HOPDs) paid through the outpatient prospective payment system, ambulatory surgical centers (ASCs) and physician offices for procedure codes that map to the Level 1 Drug Administration APC in 2022.3 Level 1 Drug Administration services includes procedure codes for administering immunotherapy injections, antigen therapies, administering influenza and pneumococcal vaccines, and other injections and infusions.
Claims were classified as urban if they contained a beneficiary state and county code that mapped to a metropolitan statistical area (MSA), and as rural if the beneficiary state and county code fell outside of an MSA.4 Using this approach, we identified how site-of-service patterns for Level 1 Drug Administration services differ for Medicare beneficiaries based on where they live:
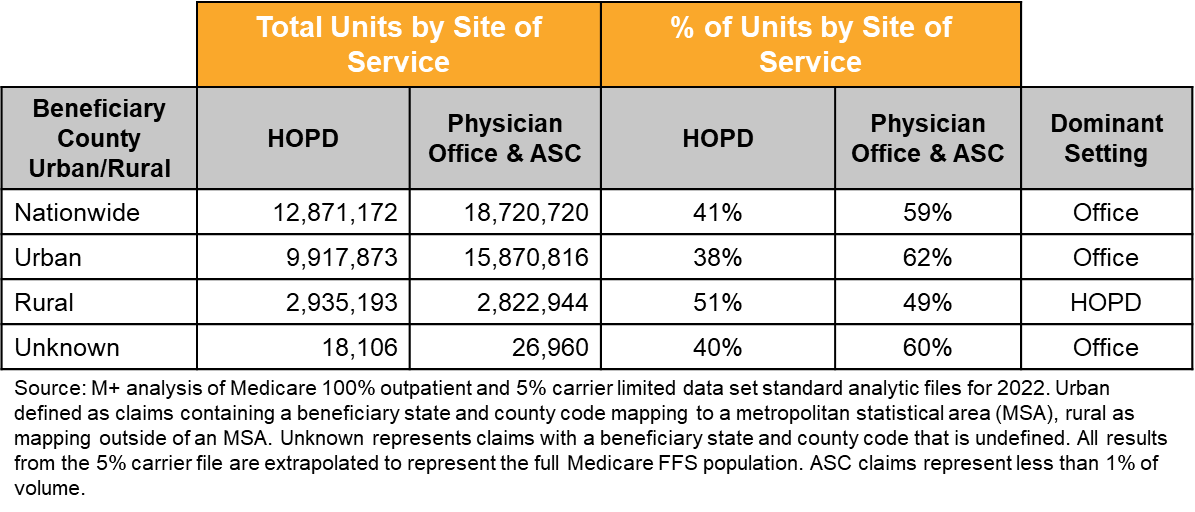
- While ASCs and physician offices are the dominant sites of service for Level 1 Drug Administration services furnished to all Medicare beneficiaries nationwide (59%) and to Medicare beneficiaries from urban areas (62%), HOPDs are the dominant site of service for beneficiaries from rural areas (51%).
- The dominant site of service for Level 1 Drug Administration services varies for beneficiaries at the county level.
As shown in Figure 1, beneficiaries living in rural areas are more likely to receive Level 1 Drug Administration services in an HOPD compared to beneficiaries living in urban areas. This reveals that HOPDs play a key role in providing patient access to these services for beneficiaries living in rural areas. Site neutral payment policies that would cut HOPD reimbursement for drug administration services – as proposed by MedPAC and Congress – could therefore have a disproportionate impact on rural beneficiaries’ access to care.
Figure 1: Total Medicare FFS Units for Level 1 Drug Administration Services in 2022, by Beneficiary County Type and Site of Service
As Figure 1 makes clear, the dominant site of service for Level 1 Drug Administration services varies. In Figure 2 below, examples of counties where beneficiaries receive more than 80% of Level 1 Drug Administration services in physician offices include: Bexar County, Texas; Hillsborough County, Florida; and Pima County, Arizona, all urban counties. Examples of counties where beneficiaries receive more than 80% of Level 1 Drug Administration services in HOPDs include: Clare County, Michigan; Patrick County, Virginia; and Drew County, Arkansas, all rural counties.
Figure 2: Dominant Site of Service for Level 1 Drug Administration Services (APC 5691)

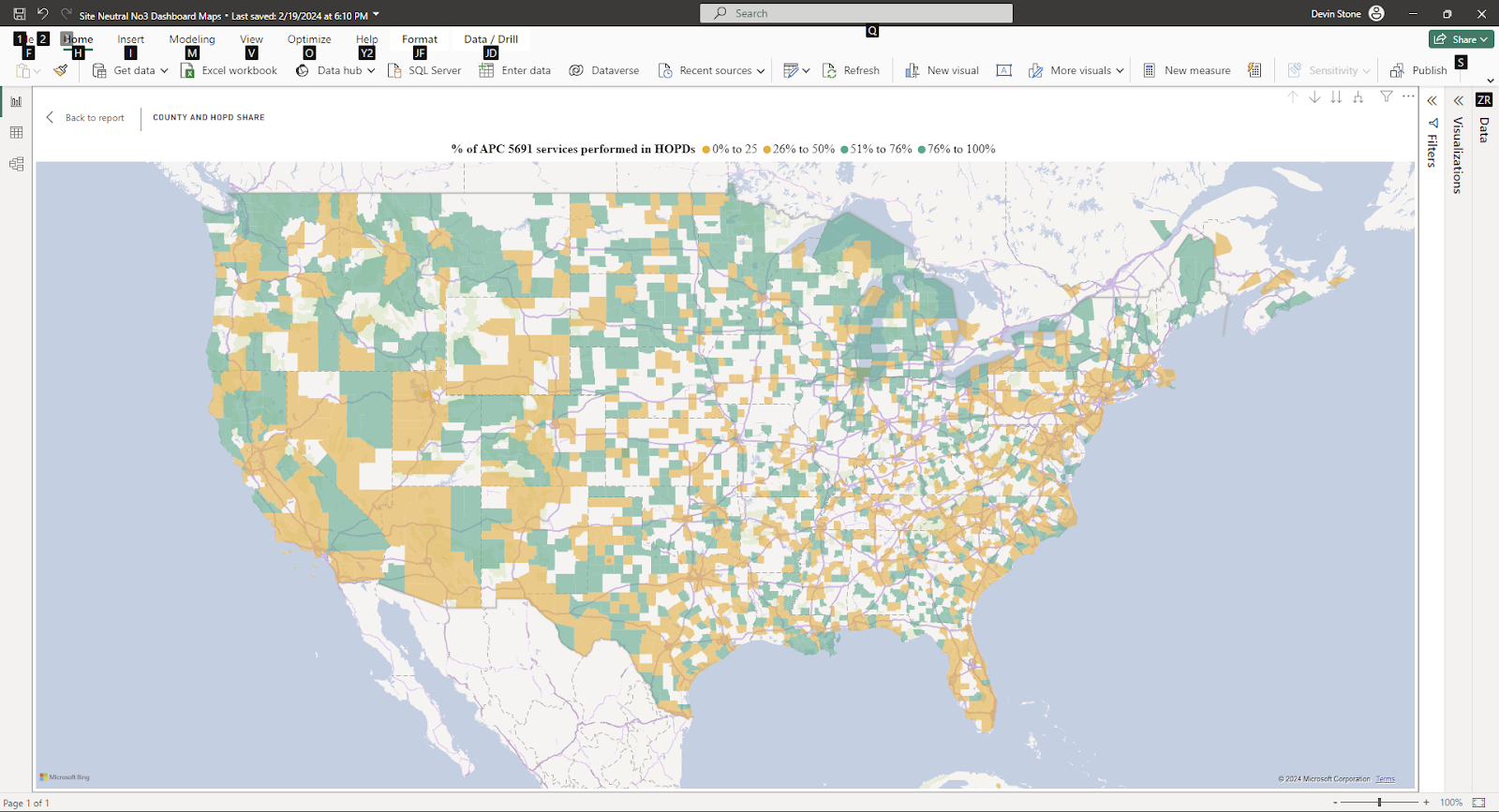
Note: Counties with 11 or fewer beneficiaries in the 5% master beneficiary file are not color coded in the above map.
Policy Implications
Site neutral payment policies for drug administration services will likely remain a key focus for federal health policymakers looking for ways to slow the growth in Medicare spending and encourage cost efficiencies. However, it is important that policymakers and stakeholders understand how site neutral payment policies for drug administration services may impact patient access, particularly for beneficiaries in rural parts of the country. Services that may be impacted includes but is not limited to administering immunotherapy injections, antigen therapies, influenza and pneumococcal vaccines, and other types of infusions and injections.
As this analysis shows, HOPDs provide over half of Level 1 Drug Administration services in rural counties. Before Congress acts to change Medicare payment policies, it should consider the potential access to care for rural beneficiaries if providers could not afford to continue to offer drug administration services in HOPD locations due to site neutral payment rate cuts.
Footnotes
[1] APC 5691, Level 1 Drug Administration; APC 5692, Level 2 Drug Administration; APC 5693, Level 3 Drug
Administration; APC 5694, Level 4 Drug Administration.
[2] The Lower Costs More Transparency Act (H.R. 5378) would limit site neutral payment reductions for drug
administration services to off-campus provider based departments of hospitals paid under the Outpatient
Prospective Payment System (OPPS) only. In contrast, MedPAC’s June 2023 site neutral payment
recommendations would apply to all HOPDs paid under OPPS, not just off-campus provider based departments
of hospitals.
[3] This analysis is limited to outpatient hospitals paid through the OPPS, ASC providers and physician offices. Our
analysis does not include drug administration services furnished in critical access hospitals (CAHs). Our analysis
shows that while CAHs are more common in rural areas, OPPS hospitals continue to bill more Level 1 Drug
Administration services than CAHs in both urban and rural areas.
[4] Less than 1% of claims had insufficient information to map to an urban or rural location.