






 i
iPolicy Update-CMS Releases FY 2022 IPPS Final Rule
On August 2, 2021, the Centers for Medicare and Medicaid Services (CMS) posted the FY 2022 Inpatient Prospective Payment System (IPPS) final rule. Effective October 1, 2021, the final rule updates Medicare payment policies and quality reporting programs relevant for inpatient hospitals, and seeks to address challenges related to the COVID-19 pandemic.
CMS stated that the FY 2022 IPPS final rule will be issued in multiple parts. The agency will address comments on proposals related to disproportionate share hospital payments, organ acquisition costs, and the Consolidated Appropriations Act, 2021 (CAA) provision concerning payments to hospitals for direct graduate medical education (GME) and indirect medical education in subsequent publications.
The final rule is available here. A CMS factsheet on the final rule is available here. The final rule is scheduled to be published in the Federal Register on August 13, 2021.
Hospital Inpatient Quality Programs and Initiatives
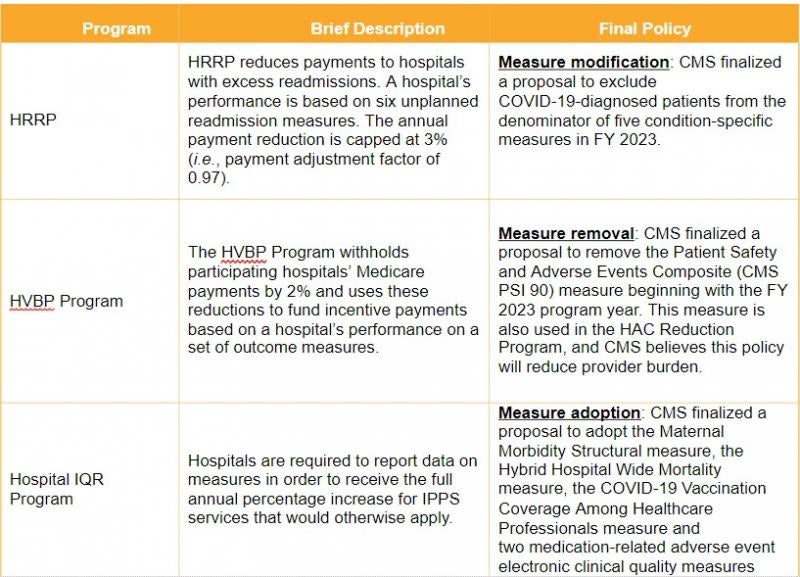
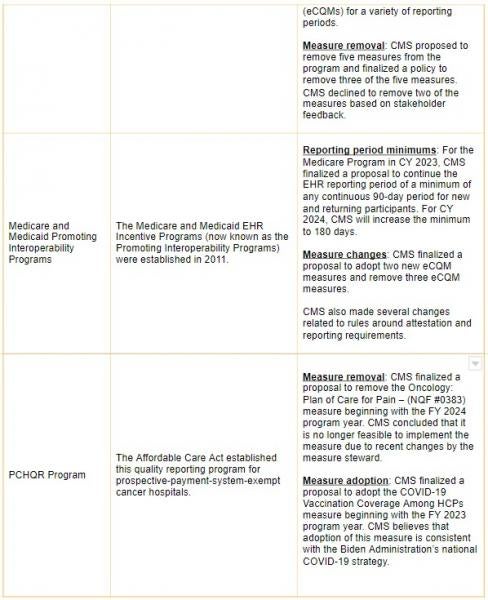
CMS monitors, rewards and penalizes quality performance in the inpatient setting through several quality incentive programs, including the Hospital Readmissions Reduction Program (HRRP), HVBP Program, Hospital-Acquired Condition (HAC) Reduction Program, Hospital IQR Program, Medicare and Medicaid Promoting Interoperability Programs, and the PPS-Exempt Cancer Hospital Quality Reporting (PCHQR) Program. These programs feature a mix of financial rewards and penalties as well as the public release of quality data.
The final rule includes several policies impacting these programs. The changes are consistent with the agency’s longstanding priority of reducing the number of quality measures (e.g., Meaningful Measures Initiative). In general, CMS sought to lessen the burden of quality reporting during the pandemic and implement policies consistent with the Biden Administration’s COVID-19 national strategy and commitment to advancing health equity.
HVBP Program
Key Takeaway: Hospitals will receive neutral payment adjustments under the HVBP Program for FY 2022.
CMS will suppress data for several quality measures in FY 2022. As a result, hospitals will receive a neutral payment adjustment under the HVBP for FY 2022.
Throughout the pandemic, CMS has implemented policies to reduce the burden of quality reporting and to mitigate negative impacts on quality scores due to pandemic-related circumstances beyond a provider’s control. In that spirit, CMS finalized a proposal to suppress data from select quality measures that the agency believes may have been impacted by the pandemic. According to CMS, these measures were not designed to accommodate changes to clinical practice that hospitals may have implemented because of COVID-19 and therefore they believe they should not impact quality scores. As a result, suppressed measures will be excluded from quality scores. The impacted measures are listed in the table below.
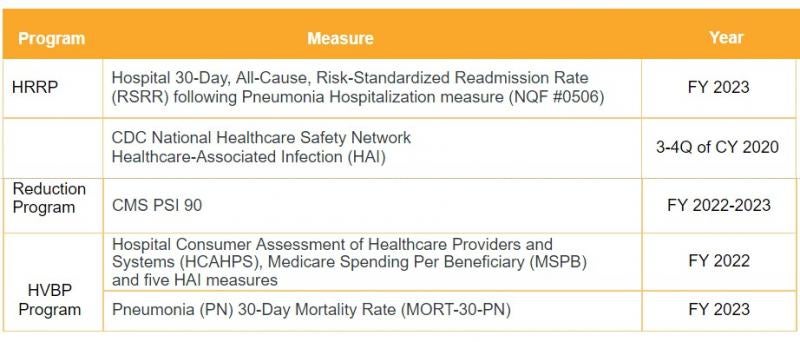
CMS believes that as a result of the data suppression, there will be inadequate data available to calculate a total performance score for the HVBP Program, and therefore CMS will not calculate such score for FY 2022. Hospitals will not be rewarded or penalized under the HVBP Program in FY 2022. Instead, CMS will ensure that value-based payments equal the amount of the reduction made to hospital’s base-operating MS- DRG payment amounts.
Adjustments to Inpatient Hospital Quality Programs and Initiatives
Key Takeaway: CMS finalized modest changes to its various quality programs. Some of these changes were made in response to the COVID-19 pandemic.
Wage Index
Low Wage Index Hospital Policy
Key Takeaway: CMS will maintain a policy that supports hospitals in low wage index areas.
Medicare payments to hospitals (and a variety of other provider types) are adjusted by a wage index intended to account for geographic differences across labor markets (e.g., the perceived cost of labor is higher in New York City than it is in rural Oklahoma). CMS updates the wage index each year based on hospital cost report data and other inputs and policies.
In FY 2020, CMS finalized a policy that boosts the wage index for hospitals with a wage index value below the 25th percentile. Affected hospitals had their wage index value increased by half the difference between the otherwise applicable wage index value for that hospital and the 25th percentile wage index value across all hospitals. CMS achieved budget neutrality for this change by adjusting the standardized amount applied across all IPPS hospitals.
CMS initially committed to maintain this policy for four years. FY 2022 will be the third of the four years the agency expects to keep this policy in effect.
Restoring the Imputed Wage Index “Rural Floor” for All-Urban States
Key Takeaway: Hospitals in four states, Puerto Rico and the District of Columbia will see a boost in their wage index resulting from legislation enacted in March 2021.
CMS calculates one wage index for each urban area and one for each rural area within each state. The Medicare statute provides that the wage index used to adjust hospital inpatient and outpatient payments for hospitals in an urban area cannot be less than the wage index applicable to hospitals in rural areas within that same state. Historically, this rule left a gap for three states that have no rural areas: New Jersey, Delaware and Rhode Island. Congress has periodically provided a patch for these three states. CMS on its own volition perpetuated this patch through FY 2018, but then allowed the policy to lapse.
The American Rescue Plan (ARP), enacted in March 2021, restored this imputed rural floor protection effective October 1, 2021, for all-urban states. In the proposed rule, however, CMS broadly interpreted the ARP change in a way that made it applicable to, and beneficial for, hospitals in Connecticut, Puerto Rico and the District of Columbia, in addition to New Jersey, Delaware and Rhode Island. CMS finalized this policy consistent with its proposal.
Wage index changes are often controversial because historically they have been implemented in a budget- neutral fashion, which means the benefit given to some hospitals comes at the expense of others. The ARP spent new money to implement this change, so the benefit to hospitals in all-urban areas will not come at the expense of others.
Urban-to-Rural Reclassification
Key Takeaway: CMS finalized changes to make it harder for hospitals to withdraw from urban-to-rural reclassification.
Medicare regulations allow hospitals geographically located in urban areas to seek to be redesignated to rural areas of their state for Medicare payment purposes. In recent years, litigation has broadened the availability and appeal of redesignation, and as a result CMS has seen an increase in the number of hospitals seeking urban-to-rural reclassification. CMS also has seen hospitals attempting to time these reclassifications to favorably impact the wage index in their state. CMS has taken steps in recent years to try to minimize these maneuvers and their impact. This year the agency proposed two technical but notable rule changes to the same effect, and finalized one of those changes.
CMS regulations will now provide that requests to cancel rural reclassifications cannot be made earlier than one year after the reclassification effective date. For example, a hospital that was approved to receive a rural reclassification effective October 1, 2021, could not request to cancel that reclassification until October 1, 2022. This change will require hospitals to maintain rural designation for at least one year before asking to cancel that designation.
CMS also proposed to eliminate the current rule that a request to cancel must be made 120 days prior to the end of the hospital’s fiscal year, and that such cancelation will be effective beginning with the hospital’s next fiscal year. CMS proposed to instead require that a hospital approved for rural reclassification (and which does not receive an additional reclassification) would have its data included in the calculation of the rural wage index for at least one federal fiscal year before the rural reclassification status could be canceled. CMS decided not to finalize this policy at this time based on comments received. The agency undoubtedly will revisit this concern and propose further changes in the future.
Transitional Stop-Loss
Key Takeaway: CMS will continue stop-loss protection for hospitals that received that protection in FY 2021.
For FY 2021, CMS provided stop-loss protection for hospitals experiencing a wage index decrease resulting from implementation of new metropolitan areas. CMS imposed a 5% cap on any decrease in a hospital’s wage index from the hospital’s final wage index in FY 2020 so that a hospital’s final wage index for FY 2021 would not be less than 95% of its final wage index for FY 2020. This was intended to be a one-time, one-year policy, but in the proposed rule CMS solicited comments on whether it should extend this policy into FY 2022 in recognition of the ongoing challenges hospitals face with regard to the COVID-19 pandemic.
CMS received comments encouraging an extension and therefore decided to extend this policy into FY 2022, but only for hospitals that received the transition protection in FY 2021. CMS will maintain budget neutrality by adjusting the standardized amount applied across all IPPS hospitals.
Graduate Medical Education
Key Takeaway: CMS deferred finalizing GME provisions to a future publication.
In the proposed rule, CMS addressed provisions to implement Sections 126, 127 and 131 of the CAA, which expanded opportunities for hospitals to receive Medicare GME funding. These provisions would have:
-
Expanded and allocated 1,000 additional Medicare-funded GME full time equivalent (FTE) resident positions over a five-year period
-
Expanded opportunities for hospitals participating in Rural Training Track programs to receive additional Medicare-funded GME FTE resident positions
-
Provided opportunities for hospitals that previously hosted residents for short rotations to receive additional Medicare-funded GME FTE resident positions and increases in their Medicare “per-resident” payment amount.
In the final rule, CMS deferred addressing these provisions to a future publication, citing the number and nature of comments received on this topic.
Rural Community Hospital Demonstration
Key Takeaway: CMS extended the rural community hospital (RCH) demonstration for five years, as required by CAA.
Legislation enacted in 2003 required CMS to establish a “demonstration” program whereby certain eligible rural hospitals would be paid under a reasonable cost-based methodology for a defined period of time. Congress has extended and expanded this program several times. Twenty-six hospitals currently participate in the RCH demonstration.
The CAA required a 15-year extension period (i.e., an additional five years beyond the current extension period). CMS proposed to extend the RCH demonstration as required by the statute and finalized a five-year extension for each of the participating hospitals. Because of the varying participation periods for the currently participating hospitals, the end date of the RCH demonstration for the hospital with the last end date will be June 30, 2028. CMS also finalized the IPPS budget neutrality calculation methodology necessary to maintain the budget neutrality of the RCH demonstration program during the CAA extension period.
Long-Term Care Hospitals
Key Takeaway: CMS made no major policy changes concerning long-term care hospitals (LTCHs).
LTCHs are acute care facilities providing care to patients with average stays of more than 25 days. LTCHs are excluded from payment under the IPPS and are instead paid under the LTCH prospective payment system. CMS routinely updates the LTCH prospective payment system concurrent with the IPPS updates. For FY 2022, CMS proposed and finalized routine payment adjustments and updates, but no major policy changes.
Changes to Medicare Shared Savings Program
Key Takeaway: CMS finalized its proposal to provide additional flexibility on the risk timeline for certain Accountable Care Organization (ACOs).
CMS finalized its policy to allow eligible ACOs participating in the BASIC track’s glide path option to forgo automatically increasing levels of risk and potential reward for performance year (PY) 2022. Under this new provision, an eligible ACO may elect to remain in the same level of the BASIC track’s glide path in which it participated during PY 2021. For PY 2023, however, an ACO that elects this deferral option will be automatically advanced to the level in which it would have participated during PY 2023 (unless the ACO elects to advance more quickly before the start of PY 2023).
Advancing to Digital Quality Measurement RFI
Key Takeaway: CMS aims to move fully to digital quality measurement in its quality reporting and value-based purchasing programs by 2025.
As part of its Meaningful Measures Framework, CMS previously outlined a path to update and align its quality measures across its different reporting programs. The proposed rule included an RFI on a four-stage plan to transition CMS’s quality measurement enterprise to be fully digital by 2025.
Comments outlined in the final rule noted general support for the movement to digital quality measures but questioned the resources and timeline necessary to fully transition by 2025. CMS did not make updates to specific program requirements on this issue in the final rule, and will address any changes in future rulemaking.
Health Equity RFI
Key Takeaway: CMS responded to comments to advance health equity in the Medicare program.
As part of the Biden Administration’s commitment to advancing health equity, and in response to the Executive Order on Advancing Racial Equity and Support for Underserved Communities through the Federal Government, the proposed rule included an RFI on how to close the health equity gap in CMS quality programs.
The Administration has included similar RFIs related to health equity in other recently proposed rules. We anticipate that the Administration in general, and CMS in particular, will continue this focus on health equity in future policy decisions.
In the proposed rule, CMS asked stakeholders to provide information about how the agency can improve reporting and application of health disparity data related to social risk factors and race and ethnicity. Specifically, the agency requested public feedback on:
-
Potential future stratification of quality measure results by race and ethnicity as well as other factors
-
Improvements to demographic data collection, including expansion of data elements and improving interoperability
-
Creation of a Hospital Equity Score in order to synthesize results across multiple social risk factors.
In the final rule, CMS responded to stakeholder comments but stated that any potential public reporting of health equity measures would be addressed in future rulemaking. The agency noted that it intended to provide future confidential feedback reports to providers on quality measure performance, broken out by race and ethnicity, but did not provide a timeline or specifics for this additional information.
Conclusion
Overall, the policies adopted in the final rule largely mirror CMS’s initial proposals. One surprise is that instead of one final rule, CMS will release additional publications to address the more than 6,500 public comments the agency received on the proposed rule. The issues that remain to be determined range from organ acquisition costs to GME funding. The delay in many ways reflects the sentiment of public comments and may be welcomed by stakeholder groups, as many of the issues are complex not only in terms of policy implication but also in terms of technicalities and implementation details.