


 />i
/>iOn February 14, 2019, the Centers for Medicare & Medicaid Services (CMS) announced its latest payment innovation model, “Emergency Triage, Treat and Transport” (ET3), which will incentivize reducing costs for the emergency transport and care of Medicare fee-for-service (FFS) beneficiaries by allowing ambulance suppliers to be paid by Medicare for transport not only to emergency departments but also to alternative sites, such as urgent care centers or primary care providers. ET3 will also pay for care provided onsite or through telehealth by qualified health care professionals.
CMS expects this model to save money by providing care in lower cost settings, and to provide care more quickly in emergency situations, where even a few minutes can make a significant difference in patient outcomes. The model may also save significant time for first responders, which could increase access to such providers.
Read on for five key takeaways from CMS’s announcement.
1. The primary participants of the ET3 model will be Medicare-enrolled ambulance service suppliers and hospital-owned ambulance providers.
Ambulance suppliers and providers participating in the ET3 model may triage Medicare FFS beneficiaries to one of the model’s interventions (e.g., urgent care center, onsite care, telehealth services) in lieu of transportation to a traditional emergency department. Patients will have the final say in their destination and could override a first responder’s decision to transport to a lesser level facility.
Local governments and other entities that have authority over 911 dispatches also may apply for funding to support the establishment of medical triage lines. With a medical triage line, individuals who call 911 would be screened to see if they are eligible for medical triage services under this model prior to ambulance initiation.
Participants will also be encouraged to partner with additional payers, including state Medicaid agencies, to provide similar interventions to all people in their geographic areas.
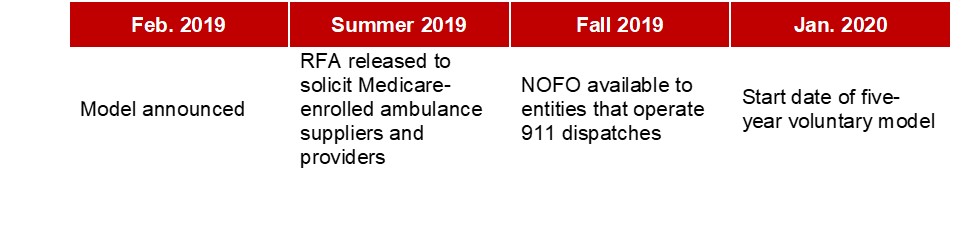
2. ET3 will launch in 2020.
The ET3 is a voluntary model and will have a five-year performance period anticipated to start in January 2020. CMS plans to release a Request for Applications (RFA) to solicit Medicare-enrolled ambulance suppliers and providers this summer.
In fall 2019, after participants have been selected and announced, the Centers for Medicare & Medicaid Innovation (Innovation Center) anticipates issuing a Notice of Funding Opportunity (NOFO) for up to 40 two-year cooperative agreements to local governments and other entities that have authority for 911 dispatches in the geographic locations where ambulance providers and suppliers have been selected to participate.
CMS is taking a staged approach to optimize overall impact with up to three rounds of RFAs, up to two releases of NOFOs, and staggered performance start dates.
3. The ET3 model has a quality component.
Participating ambulance suppliers and providers earn up to a 5 percent payment adjustment in later years of the model based on their achievement of key quality measures. Limited information is currently available on the model’s quality component, but CMS has indicated that it will aim to avoid adding more burden on participants, including by minimizing any new reporting requirements.
4. CMS estimates $1 billion in savings from ET3.
The savings will come primarily from reduced emergency department and hospital admissions. The agency estimates that up to 19 percent of Medicare FFS beneficiaries who currently access emergency ground transportation services could be treated at home or in another lower acuity/lower-cost setting.
5. The ET3 model is consistent with the Trump Administration’s larger innovation strategy and priorities.
As we pass the halfway mark of President Trump’s first term, the ET3 model joins other administration efforts to rethink incentives around care delivery with a focus on reducing costs, enhancing quality and improving patient choice. Other recent administration efforts have focused on controlling prescription drugs prices, encouraging the use of bundled payment models (Bundled Payments for Care Improvement Advanced) and modernizing the Medicare Advantage program (Medicare Advantage Value-Based Insurance Design Model). It is worth noting that while Secretary Azar and others in the administration have indicated support for the implementation of mandatory models, the ET3 is a voluntary model.
The ET3 will be implemented by the Innovation Center, which was established to support the development and testing of health care payment and service delivery models. Click here for the McDermottPlus CMS/CMMI Payment Model Tracker.