






 i
i|
Introduction Site neutral payment proposals are currently a key topic among policymakers. This +Insight explores how Medicare fee-for-service (FFS) site-of-service patterns vary across states and metropolitan statistical areas (MSAs). Our previous +Insights from February 2024 and March 2024 examined how site-of-service patterns vary across individual procedures that map to the same ambulatory payment classification (APC), and how they vary across rural and urban markets. We also analyzed services that are likely to be targets in site neutral payment proposals in our June 2023 +Insight. Key Takeaways:
|
BACKGROUND
In June 2023, the Medicare Payment Advisory Commission (MedPAC) recommended that Medicare reduce hospital outpatient department (HOPD) and ambulatory surgical center (ASC) payment rates for 66 APCs. MedPAC selected these APCs because nationally, these services were furnished in ASCs or physician offices more than 50% of the time, suggesting that they could safely be provided in lower cost settings. Cutting HOPD and ASC payment rates to align with the lowest cost setting in which the service can be provided safely is consistent with MedPAC’s belief that “Medicare should base payment rates on the resources needed to treat patients in the most efficient setting.”1 However, our analysis shows that Medicare FFS utilization and practice patterns vary across communities and are not always consistent with national trends.
DOMINANT SITE OF SERVICE VARIES BY GEOGRAPHY
APCs Where MedPAC Recommends Aligning HOPD and ASC Payment Rates with Physician Office Payment Rates
To better understand the potential impact of MedPAC’s recommendations, McDermottPlus created a stratified analysis based on where Medicare beneficiaries live, which allows us to understand how local utilization and practice patterns differ from the national trends identified by MedPAC. We analyzed the 5% Part B carrier (physician and ASC claims) and 100% outpatient hospital claims for a nationally representative sample of Medicare FFS beneficiaries to determine the dominant site of service by APC, state and MSA.2 All analysis was limited to the 66 APCs singled out by MedPAC for payment rate reductions, and the state and MSA were defined for each patient based on the county where the beneficiary resides. Stratifying the analysis based on where Medicare beneficiaries live allows us to understand how local utilization and practice patterns differ from the national trends identified by MedPAC.
MedPAC recommended that HOPD and ASC payment rates for 57 APCs be reduced to align with physician office payment rates because nationally, these services are furnished in physician offices more than 50% of the time. For example, nationally, the physician office is the dominant site of service for APCs 5691 and 5692, which describe Level 1 and Level 2 drug administration services, respectively.3 However, our analysis shows that the dominant site of service for these APCs varies at the state level. For APC 5691, the HOPD is the dominant site of service for beneficiaries in 21 states, and for APC 5692, it is the dominant site of services for beneficiaries in 20 states, as described below in Table 1.
Table 1. Differences in Dominant Site of Service by Beneficiary State Code Listed on Claim – HOPD Versus Physician Office, APCs 5691 and 5692

Source: McDermottPlus analysis of Medicare 100% outpatient and 5% carrier limited data set (LDS) standard analytic file for 2022. Results from the 5% carrier file are extrapolated to represent the full Medicare FFS population. Dominant setting defined as the setting responsible for more than 50% of services billed. State determined based on beneficiary state code listed on the claim.
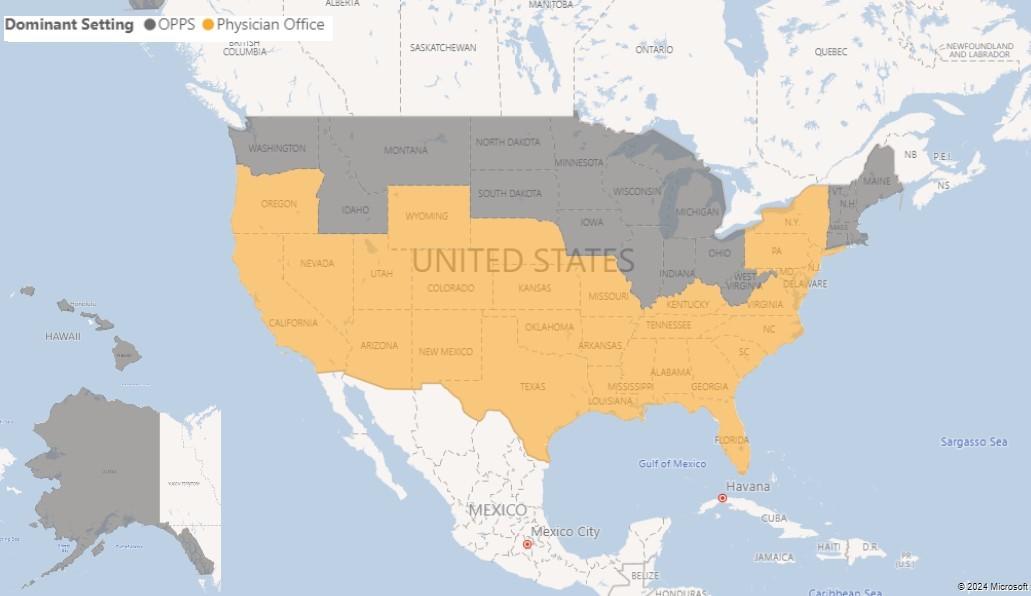
The map below (Figure 1) further illustrates the variation in site of service by state. For example, while HOPDs are the dominant site of service for APC 5691 for beneficiaries living in Wisconsin and Minnesota, physician offices are the dominant site of service for beneficiaries living in Arizona and Texas.
Figure 1. Dominant Site of Service by Beneficiary State Code Listed on Claim, APC 5691
Source: McDermottPlus analysis of Medicare 100% outpatient and 5% carrier LDS standard analytic file for 2022. Results from the 5% carrier file are extrapolated to represent the full Medicare FFS population. Dominant setting defined as the setting responsible for more than 50% of services billed. State determined based on beneficiary state code listed on the claim.
APCs Where MedPAC Recommends Aligning HOPD Payment Rates with ASC Payment Rates
MedPAC identified nine APCs that are most commonly performed in ASCs and recommended that HOPD payment rates for these services be aligned with ASC payment rates. For example, nationally, the ASC is the dominant site of service for APCs 5311 and 5312, which describe Level 1 and Level 2 lower GI procedures, respectively. However, our analysis shows that in more than half of states, HOPDs are the dominant site of service for these APCs, as shown below in Table 2. This suggests that the national trends cited by MedPAC were likely driven by high-density service areas where ASCs are the dominant site of care.
Table 2. Differences in Dominant Site of Service by Beneficiary State Code Listed on Claim – HOPD Versus ASC, APCs 5311 and 5312

Source: McDermottPlus analysis of Medicare 100% outpatient and 5% carrier LDS standard analytic file for 2022. Results from the 5% carrier file are extrapolated to represent the full Medicare FFS population. Dominant setting defined as the setting responsible for more than 50% of services billed. State determined based on beneficiary state code listed on the claim.
*Note: For APC 5311, one state had dominant site of service as physician office.
To understand how practice patterns vary across markets, we looked at practice patterns by MSA based on the county where the beneficiary lives, then ranked these MSAs by their total volume of services for APCs 5311 and 5312. For beneficiaries living in MSAs with a higher volume of services for APCs 5311 and 5312, the ASC was often the dominant site of service. For example, for beneficiaries living in the top 10 MSAs by total volume of APC 5312 services, the ASC was the dominant site of service in six MSAs. On the other hand, for beneficiaries living in MSAs with lower volumes of APCs 5311 and 5312, a greater share of services were furnished in HOPDs. For example, beneficiaries living in the 10 MSAs with the lowest volume of APC 5312 services, the HOPD was the dominant site of service in six MSAs. The map below (Figure 2) shows the dominant site of service for APC 5312 based on where beneficiaries live.
Figure 2. Dominant Site of Service by MSA Associated with Beneficiary State and County Code Listed on Claim, APC 5312
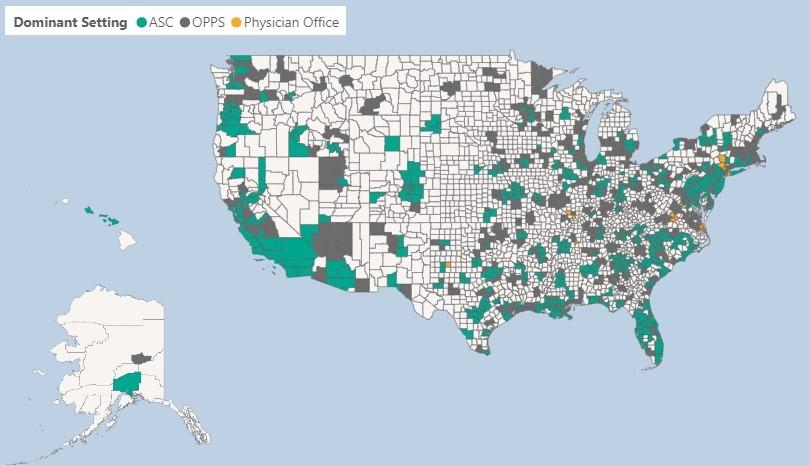
Source: McDermottPlus analysis of Medicare 100% outpatient and 5% carrier LDS standard analytic file for 2022. Results from the 5% carrier file are extrapolated to represent the full Medicare FFS population. Dominant setting defined as the setting responsible for more than 50% of services billed. MSA determined based on beneficiary state and county code listed on the claim.
KEY POLICY AND ECONOMIC CONSIDERATIONS FOR SITE NEUTRAL PAYMENT PROPOSALS
While site neutral payment proposals could potentially decrease beneficiary cost-sharing and save money for the Medicare program,5 it is important for policymakers to consider that national policies may have different implications across local communities. In areas of the country where physician office and ASC access is more limited, HOPDs may play an important role in maintaining beneficiaries’ access to critical services. It will be important for policymakers to understand the clinical, economic and patient access issues that could arise at the state, MSA and county levels as a result of site neutral payment policies.
Footnotes
[1] MedPAC. June 2023 Report to Congress, Chapter 8. “Aligning fee-for-service payment rates across ambulatory settings.” Accessed Jan 2024.
[2] This analysis was limited to outpatient hospitals paid through the OPPS, ASC providers and physician offices. Our analysis does not include services performed in critical access hospitals.
[3] APC 5691, Level 1 drug administration; APC 5692, Level 2 drug administration.
[4] APC 5311, Level 1 lower GI procedures; APC 5312, Level 2 lower GI procedures.
[5] Adler, L., Fiedler, M., & Ippolito, B. (2023). Assessing recent health care proposals from the House Committee on Energy and Commerce.